This leaflet provides you information about your surgery. The information in this leaflet should already have been explained to you by a Doctor. We hope this helps you remember what you discussed with your Doctor and also to answer any questions you may have. If you still have questions after reading this leaflet, then please contact a member of the team.
Why do I need surgery for Ovarian Cancer?
You have either had results of tissue samples (biopsies) indicating that you have an ovarian/primary peritoneal or fallopian tube cancer (this will be referred to as ovarian cancer for the rest of this leaflet), or a CT scan suggesting a high likelihood of ovarian cancer. Ovarian cancer is normally treated by a combination of surgery and chemotherapy. For some patients with ovarian cancer the surgery is performed first (primary surgery), followed by chemotherapy, while for other patients they will have chemotherapy before and after the surgery when the surgery becomes known as ‘interval debulking surgery’.
Your medical team feel that now is the right time to attempt to remove as much of your ovarian cancer as possible through surgery. Surgery for ovarian cancer is the same whether it is ‘primary surgery’ or ‘interval debulking surgery’ only the timing of when to do the surgery changes.
What happens during surgery for Ovarian Cancer?
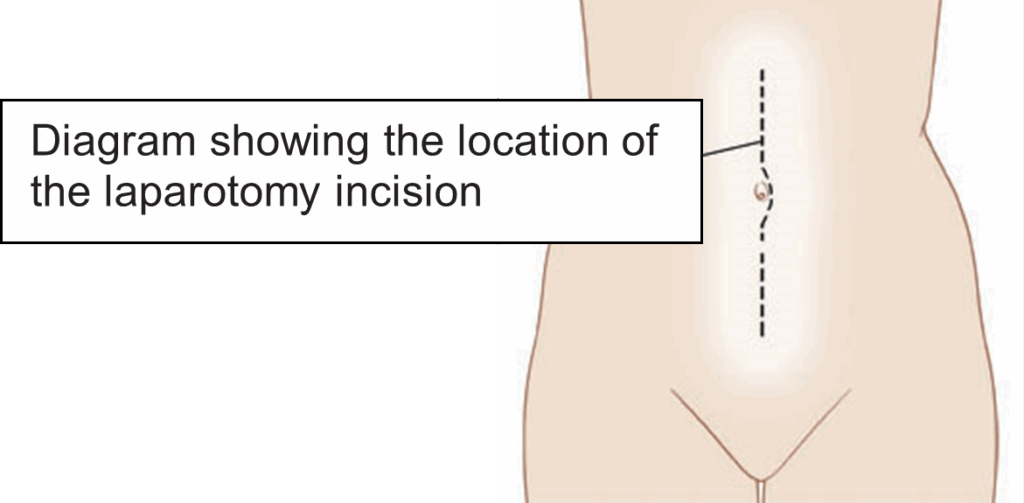
The name for this type of surgery is a laparotomy. A laparotomy is done under a general anaesthetic (you are asleep during the surgery). The surgeon will make an up and down incision (cut) on your abdomen (tummy) starting at the top of the pubic hair line and going up to, and sometimes beyond the belly button (umbilicus).
The exact surgery depends on what the surgeons finds but this usually involves removal of:
- Both ovaries
- Both fallopian tubes
- Removal of the womb and neck of the womb (hysterectomy)
- Removal of the omentum. The omentum is a pad of fat that hangs over the front of the stomach and is a common place for ovarian cancer to spread to.
The aim of the surgery is to remove as much cancer as possible (ideally all visible cancer) and in some cases may involve removal of tumour (cancerous growth) from the diaphragm (muscle that separates the chest from the abdominal cavity), removal of the appendix and spleen. If the spleen is removed you will need to have additional vaccinations and take lifelong antibiotics. In some cases the surgeon may need to remove deposits of disease from the liver surface.
All patients having surgery for ovarian cancer will have the possibility of bowel surgery discussed with them. This is either because there may be an injury to the bowel during surgery, or because the bowel is involved with cancer, and in order to remove the cancer the surgeon has to remove part of the bowel. The surgeon may be able to re-join the ends of the bowel once the section that was injured/involved with disease is removed. This is called an anastomosis.
Occasionally it is not possible or not safe to re-join the bowel and instead the end of the bowel is pushed through the abdomen out onto the skin to form a stoma (see pictures below). This lets your stool (bowel contents) empty into a stoma bag which is attached onto your skin.

A stoma can be permanent or be reversed in some patients in the future with a smaller surgery. The chance of having a stoma is about 10-15% and most patients do not require this extra bowel surgery. It is uncertain before the surgery if a stoma is required. If identified as a candidate for bowel surgery, you will see a nurse who specialises in the care of people with stomas (called a stoma nurse). They will explain about stomas and answer any questions you have about them. After examination they will use a skin marker to apply two black dots to your tummy. After the surgery, the stoma nurse will teach you how to look after your stoma and give you information and support to help you cope with any problems.
On a small number of occasions the surgeons finds that removing the cancer is too dangerous for the patient and may not be able remove much cancer during the surgery.
What are the alternatives to not having surgery?
If you feel that you do not want to have surgery other options will be discussed with you by your medical team. Surgery alone is often not enough to treat ovarian cancer and you may be required to have chemotherapy.
Can there be any complications or risks associated with this surgery?
Before you have your surgery you will be told about the risks of the surgery and you will be asked to sign a consent form which will list the potential risks. Please ask questions at any time. More ‘serious’ complications can include:
- General anaesthetic carries a small chance of complication. This will be discussed with your anaesthetic doctor before your surgery. It is important to realise that these risks and complications are rare and every care is taken to keep the risks as low as possible.
- Infection- The risk of after surgery infections is reduced by giving ‘preventative’ antibiotics around the time of surgery but infection can still sometimes occur in the chest, wound, pelvis or urine. Infections are usually easily treated with antibiotics.
- Bleeding (haemorrhage) – This may occur during the surgery or rarely afterwards. Blood transfusion is required in around one in five surgeries. You may need to return to theatre in the rare case of internal bleeding after the surgery.
- Injury to the ureters – the ureters carry the urine from the kidneys to the bladder. The ureters can be damaged at the time of the surgery due to being so close to where the cancer is being removed. This damage will be repaired during the surgery. Some people may have some difficult passing urine after the surgery, this may mean needing a catheter in your bladder for a period of time. This is usually only for a few days but sometimes longer.
- Clots (thrombosis) – It is possible for clots of bloods to form in the deep veins of the legs and pelvis, this is called a deep vein thrombosis (DVT). This will normally cause pain and swelling in the affected leg and is relatively simply to treat using blood thinning drugs. In rare cases it is possible for a clot to break away and be deposited in the heart or lungs. If this occurs it is a potentially serious complication but several measures will be taken to reduce the risk of this happening. Moving around as soon as possible after your surgery can help as can wearing special surgical stockings and having injections to thin your blood.
- With every surgery there is a very small risk of death.
More common complications that can occur from this surgery
- Anaemia
- Fatigue / tiredness
- Urinary frequency or loss of control
- Numbness, tingling or burning sensation around the scar which may take weeks or months to resolve.
- Pain/discomfort
- Bruising
- Delayed wound healing
- Scarring of the skin or scar tissue inside (adhesions)
Consequences of treatment
Following your surgery you may experience some of these problems. Your medical and nursing teams are available to support you and to help to address any problems that may occur.
- Leg swelling (lymphoedema) – In some cases when the lymph nodes are removed. This is a build-up of lymph fluid which mostly affects the legs. It can develop in other body areas such as the abdomen (tummy area), genitals and pelvic area. If this were to occur you would be referred to a nurse led lymphoedema clinic.
- Menopause (if not already menopausal) – some of the main physical effects are vaginal dryness, hot flushes, mood changes and low libido (sex drive). This occurs when your ovaries are removed so your hormone levels reduce quickly. How long these symptoms last for is different for everyone. In some cases women can start hormone replacement therapy however this will depend on the outcome of your surgery.
- Effects on sexual functioning (discomfort, bleeding, reduced libido)
- Emotional/social consequences of diagnosis and treatment
- Change in bladder/bowel habit
When can I have sex?
Following surgery for cancer, you may not feel physically or emotionally ready to start having sex again for a while. We normally advise women not to have sexual intercourse for 6 weeks following surgery. During this time, it may feel important for you and your partner to maintain intimacy, despite refraining from sexual intercourse. However, some couples are both physically and emotionally ready to resume having sex much sooner and this can feel like a positive step. If you have any worries or concerns, please discuss them with the Gynaeoncology CNS. It can be a worrying time for your partner. He or she should be encouraged to be involved in discussions about the surgery and how it is likely to affect your relationship afterwards. If you do not have a partner at the moment, you may have concerns either now or in the future about starting a relationship.
Please do not hesitate to contact the gynaecology CNS if you have any queries or concerns about your sexuality, change in body image or your sexual relationship either before or after surgery.