In-vitro fertilisation (IVF) is a fertility treatment that involves the use of drugs to stimulate the ovaries into producing eggs. The eggs are then taken out of the body and fertilised in the laboratory. The fertilised egg(s), which are called embryos, are then replaced in the uterus (womb).
IVF was originally designed to treat couples where the fertility problem was caused by blocked fallopian tubes and this is still the main indication for IVF.
However, IVF is now used to treat a variety of fertility problems, including:
- Endometriosis
- Mild to moderate degrees of sperm abnormality
- Unexplained infertility
- Ovulation problems
- No male partner
There are a number of stages involved in the IVF process and this booklet aims to guide you through each stage:
- Pre-treatment counselling
- Consent
- Downregulation
- Superovulation
- Egg Collection
- Sperm Collection
- Fertilisation & Division
- Embryo Development and the EmbryoscopeTM incubator
- Embryo Transfer
- Embryo Transfer Policy
- Embryo Freezing
- Problem with IVF
- Contact us
1. Pre-Treatment Counselling
Before you attend Gateshead Fertility Unit for the first time you will have had investigations carried out to diagnose why you have not fallen pregnant. If IVF is thought to be the most appropriate treatment you will be contacted by the Fertility Unit to organise your IVF cycle. The Fertility unit will send you an appointment to attend for investigation which will determine the most suitable treatment. At this appointment you will receive an information pack which will contain a date and time for your consent consultation as well as the following documents;
- Unit Information Booklet
- IVF Patient Information Booklet
- ICSI Booklet
- Counselling Information
- Information on Legal Parenthood
- Embryo Transfer Policy
- Information relating to welfare of the child assessment
- Unit success Rates
- Multiple Pregnancy Information
- Price list – for couples funding their own treatment
You will already have completed GDPR and marital status forms. On receipt of these you will then receive an SMS message on how to access the relevant consent forms for your treatment.
Before your consent consultation is carried out, it is important that the following investigations have been completed:
- Sperm Test – this is an important test as it allows our embryologist to prepare the sperm in a special way, similar to that which will happen on the day of treatment. We have a private room in which to produce the sample and this allows the sample to be assessed and prepared immediately.
THIS TEST MUST BE CARRIED OUT, AT THE LATEST 1 WEEK PRIOR TO YOUR APPOINTMENT.
(If you have had a semen analysis at Gateshead fertility unit within the last 6 months you may not need to repeat the test. Please contact the unit to discuss this.)
b. Blood Tests
- The female egg provider will need an AMH (Anti Mullerian hormone) test. This hormone level will inform us of your ovarian reserve and will help indicate how sensitive your ovaries will be to the fertility drugs. This also allows us to calculate the starting dosage of fertility drug. This blood test can be performed at any time of your cycle but may take up to 1 week for the results to be available. We will also obtain bloods for screening HIV, Hepatitis B, Hepatitis C and Rubella. You may have had your AMH and rubella checked previously so these may not need repeating.
- If the male partner is providing a sperm sample then HIV, Hepatitis B and Hepatitis C blood tests are also obtained. This can be arranged for the same appointment time as the sperm test or at another pre-arranged time, again this must be at least a week before your individual consultation to allow results to be discussed (for more information please see ‘blood tests’).
- Consents – The online consents need to be completed at least 2 days prior to your consultation. The electronic-consent platform (Fertility Consent) consists of videos explaining the treatment and then the relevant consent forms to be completed. These can take up to 2 hours to complete. You will also require a valid photographic ID e.g. passport or driving license and your NHS number. If the consent forms are not completed in time for your consultation, then the appointment will need to be cancelled and rearranged.
At your Consultation you will be able to discuss the individual circumstances of your treatment with the medical staff. You will have the opportunity to discuss any concerns that you have and ask any questions. The doctor will go through all of the consent forms with you to ensure that they are correctly completed and accurately reflect your wishes.
We will also need to carry out the following investigations:
- Ultrasound Scan – all scans during the fertility treatment are performed trans-vaginally. This means that a thin lubricated ultrasound probe is inserted (approximately 2 inches) into the vagina to allow the doctor to see the ovaries and uterus. This will help us to assess whether the uterus is normal and allow us to measure the size of the uterus so we can accurately place the embryos in the womb at time of embryo transfer. We will also be able to ensure that the ovaries are normal and accessible for egg collection.
THIS SCAN WILL BE PERFORMED AT YOUR INITIAL CONSULTATION - Screening Tests – We will ask the female egg provider for two vaginal swabs to test for Chlamydia and other infections, you will be able to do this yourself.
- Catheter Test – This test may be performed if you have had treatment to the cervix in the past or have had a difficult transfer elsewhere. The catheter test is very similar to the embryo transfer and feels like a smear test. Firstly, a speculum is inserted into the vagina and the cervix is cleaned with a piece of cotton wool. A fine soft plastic catheter is then fed gently through the cervix. This test allows us to determine the passage to the womb and make the embryo transfer as easy as possible.
- Prescriptionsfor your medication will also be given at this appointment. You will need to collect these from the hospital pharmacy (normal prescription charges apply). It is worth considering a pre-paid prescription which covers all NHS prescriptions for 3 months and it will save you money. If your fertility treatment is on a private basis, the drugs may be purchased at the hospital pharmacy or dispensed by the home care system (see separate leaflet).
The nurses will reiterate the important aspects of the treatment and give information about our counselling service. They will also coordinate the dates for your treatment and teach you how to administer your own drugs.
2. Consent Forms
There are 2 consent forms for each partner which can be completed prior to your attendance at the IVF unit. These forms will be explained to you on the online electronic- consent platform (Fertility Consent). The forms relate to;
- Consent to disclose information about your treatment to your GP and other members of staff. Consent to contact and non-contact research via the HFEA.
- Consent to the use and storage of your sperm, eggs and embryos
Consent forms are designed to protect your wishes and we cannot use or store your eggs, sperm or embryos without your permission.
Consent to Disclose Information
By law, we need your consent to disclose information about your treatment to your GP or other medical or administrative staff.
Information about all IVF treatment cycles carried out in the UK is held both at the clinic where the treatment is carried out and also centrally at the HFEA. This will include information such as how many eggs were collected, how many embryos were transferred, what the outcome of treatment was and the outcome of any pregnancies etc.
This means that the HFEA hold a huge amount of information about IVF treatments. This information can be useful to organisations researching IVF treatments. The HFEA are asking permission from you for this non identifying information to be able to be used to help aid research about fertility.
Consent to the use and storage of sperm, eggs and embryos
We need your permission to use and store your eggs, sperm and embryos. You will be asked if you consent to your eggs, sperm and embryos being “used” for your own treatment (i.e., in IVF), donated to other people and/or used for research. These options will be discussed fully with you before you sign the consent form.
It may be possible to “store” or freeze spare embryos at the end of your treatment. However, we need the consent to store embryos from both partners*. Please be aware that the initial period for storage is up to 10 years. It is possible to renew the storage consent beyond 10 years and you will receive more information during your treatment. We will discuss the option of freezing embryos and consent at your consultation and after embryo development. In some cases, we may recommend storing sperm before treatment. We do not currently offer egg storage.
It is important to be aware that there is a remote possibility of damage or loss of stored material during the process of freezing, storing and thawing.
You should be aware that any consent regarding the use and storage of embryos/ gametes can be changed or withdrawn at any time. This is until the point where the gametes/ embryos have been transferred to a patient in the course of treatment or used in a project of research. If you wish to change your consent form, then you should contact the unit. In the case of frozen (stored) embryos, changing your consent may have implications for your partner. If one partner no longer wishes for the embryos to remain in storage, then the embryos must legally be removed after a 12 month ‘cooling off’ period.
Any consent must include a statement of what should happen to the stored embryos or sperm should you die or become mentally incapacitated. You may want to allow your partner to use the sperm or embryos. You may want to allow the sperm or embryos to perish or be donated to research or another couple. We will discuss all these options at your appointment.
Effective consent must be “informed”. If you are not sure about the procedures you are about to undergo or have any confusion surrounding your consent form, please discuss it with a member of staff.
* If donor sperm or eggs was/were used to create the embryos the donor must have consented to the freezing of embryos.
All of the consent forms have a page declaration at the bottom of each page, these must all be signed and dated and appropriate passport/ NHS numbers entered correctly, please do not sign any consent if you do not fully understand the implications of that consent.
Further consent forms to sign relate to the actual IVF treatment cycle itself and the Doctor will complete this with you at your appointment and a research/ training consent.
3. Downregulation
Downregulation involves switching off the pituitary gland. The pituitary gland produces hormones to control the menstrual cycle. We need to switch off these hormones to stop them interfering with the IVF cycle. Downregulation must be continued until staff informs you to stop.
The types of drugs used in downregulation are:
- Naferelin (Synarel)
- This is a nasal spray. You must have 2 sniffs in the morning and 2 sniffs in the evening (one in each nostril twice a day). This isn’t suitable if you suffer from nasal problems e.g., hay fever.
- Buserelin (Suprafact)
This is a daily injection which is to be administered in the morning. We will teach you how to give yourself these injections before starting. - Prostap
- This is an injection which is given twice, 1 month apart. This can be given by the nursing team or you can do it yourself. A QR code which takes you to a video will be given to assist you.
These drugs can be started irrelevant of where you are in your cycle. You will be given a start date at your consultation.
Risks and Side Effects
Because the down regulation drug switches of your hormones, you may experience a number of menopausal-like symptoms such as: hot flushes, irritability and headaches.
Immediately after starting the downregulation drugs, a burst of your own hormones may be released, this could increase your fertility for a few days. It is therefore advisable that you use a barrier method of contraception until your next period or scan as it puts you at risk of a multiple pregnancy.
Antagonist
It may be decided to use a protocol that means you don’t have the downregulation drug. This is called an Antagonist protocol and may involve you starting injections with your period or even having the oral contraceptive pill for 2-3 weeks before starting the FSH injections. A daily injection called FYREMADEL/ CETRORELIX is the antagonist that is used alongside the superovulation drug.
Your individual protocol will be discussed with you at your appointment
STEP BY STEP:
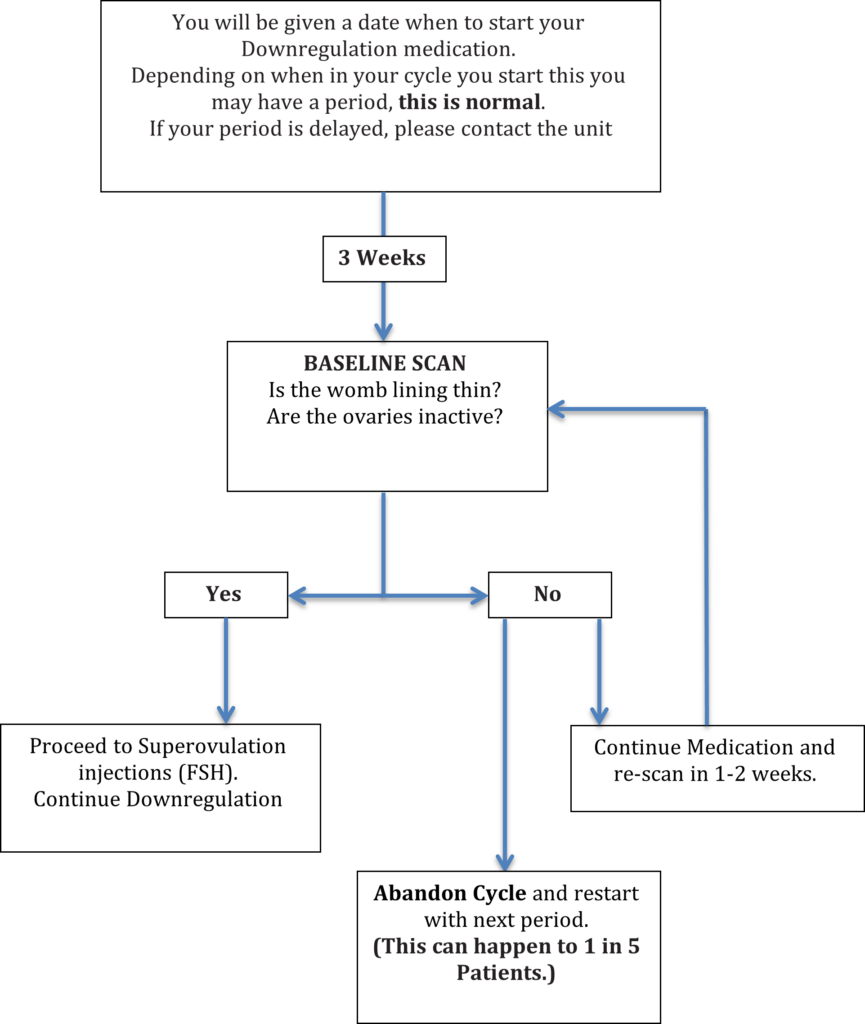
4. Superovulation
During this part of the cycle, we use fertility drugs to stimulate your ovaries into producing a number of eggs.
It is important you continue the downregulation drugs during this part of the cycle.
The type of drug used in superovulation is a hormone called follicle stimulating hormone (FSH). This is a daily injection which is to be administered in the evening. We will teach you how to give yourself this injection before starting. We may use a drug called OVALEAP/ MERIOFERT. The choice of drugs will be discussed with you before you start treatment.
It is essential that we monitor the growth of the follicles and we do this with the day 6 and day 10 scans, occasionally we may perform blood tests.
Risks and Side Effects
As you will be giving yourself daily injections you may experience some bruising at the injection site.
The aim of superovulation is to stimulate the ovaries into producing follicles. If too many follicles develop you may develop Ovarian Hyperstimulation Syndrome (OHSS). This is discussed in detail later in this booklet.
STEP BY STEP:
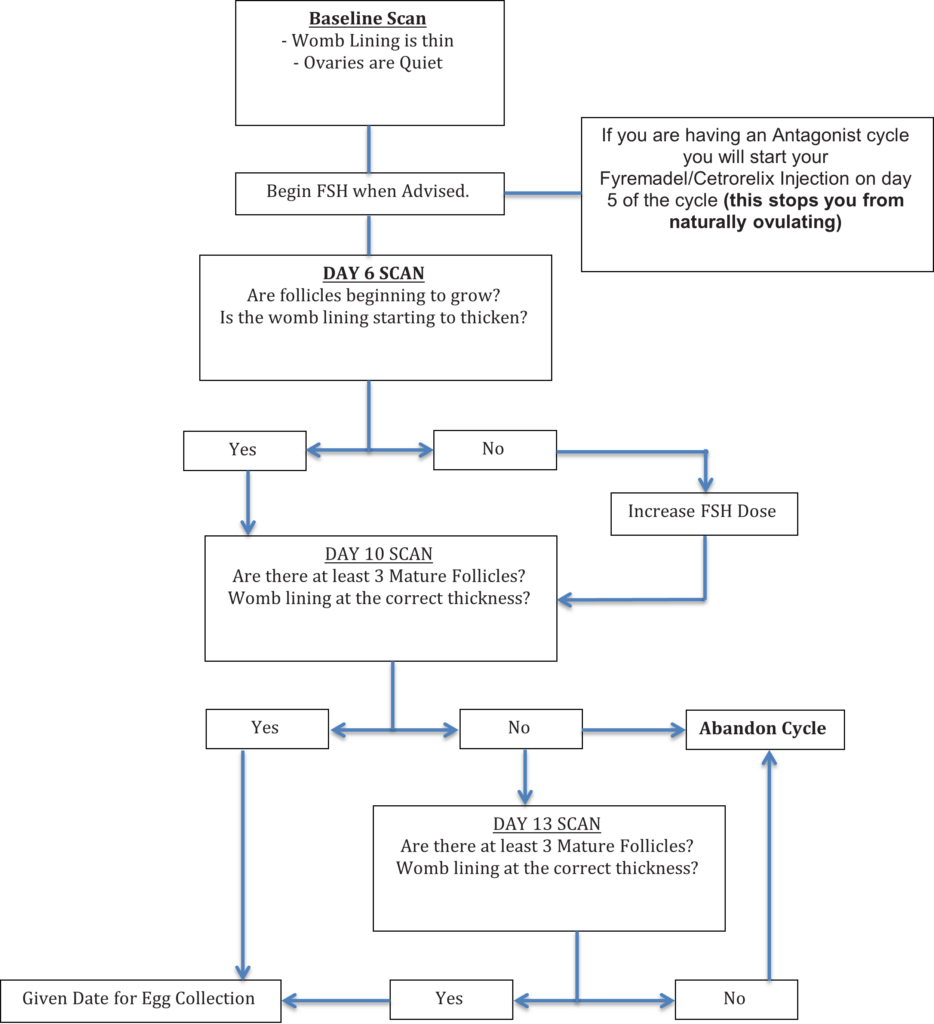
5. Egg Collection
If at least 3 mature egg follicles have grown and the womb lining is suitably thickened, we can collect the eggs. Firstly, you have a final injection Gonasi – human chorionic gonadotrophin (hCG), which matures the eggs. 36-38 hours after this injection we collect the eggs. If we attempted an egg collection later than this (40+ hours) ovulation may have occurred and we would have lost the eggs. The timing of this injection and egg collection are therefore very important. You will be given detailed information about the egg collection during the treatment cycle.
The procedure itself is performed within our IVF theatre using the vaginal scanner with a fine needle attached. The needle is passed into each ovary and the fluid filled follicles that hopefully contain the eggs are drained and passed to the embryologist in the laboratory. Once collected, the eggs are washed and stored in the incubator. On average an egg is collected from 80% of follicles. The whole procedure lasts approximately 15 minutes and a mixture of sedatives and painkillers are used to ease the discomfort/pain of the procedure.
6. Sperm Sample
We ask that you abstain from intercourse or ejaculation for 2-3 days – this allows the correct build-up of sperm.
IT IS IMPORTANT TO AVOID SEXUAL INTERCOURSE TO PREVENT THE POSSIBILITY OF SPONTANEOUS CONCEPTION.
The sperm sample is collected after the egg collection. Ideally this sample should be produced in the hospital – we have a private room for this. To avoid contamination, we ask that the men wash their penis before producing the sample using non-perfumed soap (e.g., simple).
You can both leave approximately 2-3 hours after the egg collection once the nurse looking after you is satisfied that you are fit to be discharged; but the women should not drive as the drugs can cause drowsiness. You will need to take the full day off work and have somebody with you at home for a 24 hour period because of the sedative drug.
7. Fertilisation and Division
In conventional IVF the prepared sperm sample is added to the eggs roughly 5 hours after egg collection. The sperm is prepared in such a way so as to inseminate the eggs with only the most active sperm. The dishes are then returned to the incubator and hopefully fertilisation will occur 3-4 hours later.
Intracytoplasmic sperm injection (ICSI) is an alternative method to fertilise eggs in cases of a severe sperm problem. There is an information booklet outlining the indications for ICSI, possible hazards and success rates.
Fertilisation can depend on a number of factors such as egg maturity and sperm function. Very occasionally the eggs can fail to fertilise.
The eggs are checked the following morning by our embryologist and you will be telephoned as soon as we know if the eggs have fertilised.
The fertilised eggs are then left in the EmbryoScope incubator overnight and should hopefully start to develop. A fertilised egg is one cell but should begin to divide to become a multi-celled embryo.
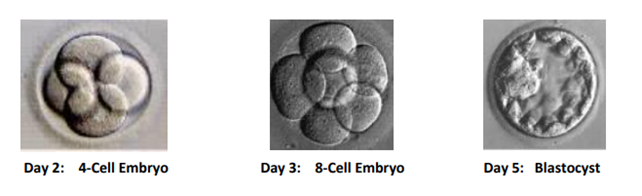
8. Embryo development and the Embryoscope™ incubator
The Embryoscope™ is a type of incubator that maintains the necessary physiological conditions required by a living embryo while they are in the laboratory. It has an incorporated time lapse system that has a camera that continuously captures images and records them as a video of the embryonic development. This system allows the embryologist to monitor embryo cell divisions while the embryos are still in the incubator, and we can carry out a comprehensive analysis of the development of the embryos.
Based on recent studies, the cell division pattern of the embryos is becoming a valid alternative for selecting the embryos which have the best potential for implantation. There is growing evidence suggesting that certain cell time points and events are especially important for predicting further development potential, and pregnancy potential of embryos. Using these time points we can choose the best embryos among all the embryos of the patient and also give a lot of information regarding the viability of those embryos.
- Information on critical time points regarding embryo development can provide our embryologists with an additional decision-making tool for embryo selection for transfer.
- Identify embryos with abnormal development patterns. Several studies have shown that embryos with abnormal characteristics may have a lower chance of implanting. We can record this information and use it to deselect those embryos with the lowest chance of implanting.
- It gives you more information about your embryo(s) and enables the embryologist to share the rationale for embryo selection thus providing a window into the laboratory.
9. Embryo Transfer
Most embryo transfers take place 5 days after the egg collection or occasionally 3 days after if only 1 embryo has developed. This decision is made by our embryology team and will be discussed with you in further detail when more information about your individual embryos is known. Then together we will decide how many embryos to replace in the womb when all information is considered. If your embryos have been stored in the EmbryoScope incubator you will also be able to view the time-lapse footage.
The Embryo Transfer policy can be found in the next section and aims to maximize the chance of a healthy live birth while minimizing the risks associated with pregnancy, such as multiple pregnancy.
The embryo transfer procedure is similar to a smear. A fine catheter with the embryo(s) is passed through the cervix and the embryo(s) is/are replaced in the womb we will scan your abdomen at the same time to ensure the embryos are replaced accurately.
We suggest that you take things easy after the embryo transfer and avoid strenuous activities and sexual intercourse for 1-2 weeks. Following the egg collection, you will need to take PROGESTERONE (this medication may be in the form of a pessary or a daily injection) these continue until your pregnancy test, progesterone keeps the womb lining healthy and receptive for an early pregnancy.
You will attend the fertility unit for a blood pregnancy test 12 days following a day 5 embryo transfer or 14 days if you have had a day 3 transfer. This gives an accurate reading of how much pregnancy hormone there is. If the result is over 200, we will arrange a pregnancy scan 2 weeks later. If the result is between 5 and 199, we will repeat the blood test 48 hours later. If the blood test is less than 5 then unfortunately the treatment hasn’t worked this time and we will offer you a follow up appointment to discuss your treatment. If you bleed before your blood test, we will still perform the test.
It is important that all patients remember that they are individuals and that outcome of treatments vary greatly and that limitations may occur according to the individual.
Success rates for IVF can be found on our results sheet.
10. Embryo Transfer policy
Our embryo transfer policy aims to maximize the chance of one health baby, while minimising the risk of a multiple pregnancy. In order to reduce the number of multiple pregnancies at our Unit, more patients are having one embryo transferred. We have found that by transferring only one embryo in carefully selected patients, the incidence of twins can be drastically reduced whilst maintaining the chance of a successful pregnancy. We will assess each patient individually looking at various factors that can influence success such as;
- The age of the egg provider
- Dose of stimulation drugs
- Number of eggs collected
- Cause of infertility
- Previous treatments and pregnancies
- Embryo quality
This individual assessment will help to predict your chance of success and risk of a multiple pregnancy. The chance of a multiple pregnancy is related to the number of embryos transferred. Our Embryo transfer policy can be found in the next section.
If you have a high chance of success (good prognosis), then the maximum number of embryos that we can replace is one, as you are at high risk of a multiple pregnancy when transferring two good quality embryos. For patients with moderate or poorer prognoses, there may be scope for transferring more than one embryo and this will be influenced by the embryo quality.
| Good-prognosis patients | |
| 1st or 2nd Cycle | Mandatory single embryo transferred (SET) on Day 5Two embryos transferred only in exceptional circumstances e.g. very poor embryo development |
| 3rd and subsequent cycles | Recommend SET on Day 5 if there are 1 or more good quality blastocysts availableConsider transferring two embryos if there are no good quality blastocysts available ORFailed implantation of 3 or more good quality embryos, including frozen embryos |
| Average-prognosis patient | |
| If 2 or more good quality blastocysts | If age is under 38 years old – SET and freeze remaining embryo(s)If age is 38 or above – discuss transferring two embryos and risk of a multiple pregnancy (MP). This will be patient choice |
| If less than 2 good quality blastocysts | Advise transferring two embryos and risk of MP. This will be patient choice. NB: Do not advise transferring two embryos if 2nd embryo is significantly lower quality than the 1st embryo |
| Poorer-prognosis patient | |
| If 2 or more good quality blastocysts | Discuss transferring two embryos or SET + embryo freezing, including risks of MP. This will be patient choice. |
| If less than 2 good quality blastocysts | Advise transferring two embryos and risk of MP. This will be patient choice. NB: Do not advise DET if 2nd embryo is significantly lower quality than the 1st embryo |
The risk of multiple pregnancies can be found in Section 12.
11. Embryo Freezing
A third of patients undergoing IVF have spare embryos of suitable quality to be frozen for you to use in the future. There is a possibility that this may be funded by the NHS; if not, there is a cost implication (please see enclosed price list).
Embryos can be frozen for up to ten years in the first instance and under certain circumstances longer. If you have the opportunity to store your spare embryos, we will counsel you fully on the risks and benefits of this procedure and obtain the necessary consent forms.
It is important to be aware that there is a remote possibility of damage or loss of stored material during the process of freezing, storing and thawing.
12. Problems with IVF
a. Unsuccessful Treatment
IVF may not work for a number of reasons:
- Failure to respond to the fertility drugs
- Technical difficulty in collecting the eggs (very rare)
- Failure of the eggs to fertilise
- The embryos do not develop normally
- Failure of the embryos to implant in the womb following transfer – this is the commonest reason that treatment fails
In many ways IVF treatment can be thought of as a series of hurdles. Every patient is different with a unique response. Unfortunately, there will always be unsuccessful treatments and this is obviously very distressing and can be difficult to cope with. It is also difficult to know when the time to stop pursuing treatment is after repeated failed treatment cycles; staff will discuss the advantages and disadvantages of continuing treatment with you on an individual basis. Our staff are always available to discuss any concerns you may have so please do not hesitate to contact us.
Counselling is available at any stage of the treatment and is free of charge. We have an independent counsellor who you may wish to talk to – all details about counselling can be found in the information leaflet about counselling and the unit booklet.
b. Ovarian Hyperstimulation Syndrome (OHSS)
Some degree of ovarian-hyperstimulation occurs in all women taking fertility drugs. However, when this over-stimulation is excessive it can lead to problems. This occurs in about 7% of women and in 2% it may be sufficiently severe to need hospital admission. Women with PCOS (polycystic ovarian syndrome) are more prone to developing OHSS and therefore need to be closely monitored.
What is OHSS?
OHSS develops when the ovaries produce too many eggs and swell up extensively. Blood vessels that supply the ovaries can leak fluid into the abdomen and cause the tummy to swell, leading to abdominal pain. Other features of the condition include vomiting which leads to dehydration. The dehydration may be made worse by fluid leaking out of the circulation, causing the blood to become concentrated. This can lead to blood clots and kidney problems. If this fluid collects in the chest, it may cause shortness of breath. It should be stressed that severe OHSS is very rare. And even in severe cases the condition is usually self-limiting and settles in a few days.
If you are worried you are developing OHSS during your treatment you must contact the unit immediately
When might OHSS occur?
- While taking the Follicle Stimulating Injections – if this occurs before the hCG injection we may stop your treatment to protect you from the effects of severe OHSS. YOU MUST NOT HAVE UNPROTECTED SEXUAL INTERCOURSE UNTIL YOUR NEXT PERIOD.
- After the hCG injection – we will collect the eggs and then offer to freeze any resulting embryos or suitable quality, to be replaced at a later date. If we replaced the embryos immediately and a pregnancy resulted, the pregnancy hormones could continue to stimulate the ovaries and make the OHSS worse. In this situation you would not have to pay for freezing embryos. The subsequent frozen embryo replacement will be counted as part of this cycle.
- During pregnancy – the hormones that are produced during early pregnancy stimulate the ovaries and can worsen OHSS
c. Multiple Pregnancy
The risk of a multiple pregnancy depends on various factors. It is more common in younger women and if the embryos are of good quality. Previous IVF history may assist us in deciding how many embryos to replace and the HFEA limits the number of embryos replaced to a maximum of 2 in women under 40 years.
Risk factors for a multiple pregnancy include:
- Female Age (younger patients have a higher risk)
- A history of previous pregnancy
- Number of good quality embryos
- Cause of infertility (higher risk for male factor infertility)
- Number of previous IVF cycles
The complications of pregnancy increase with multiple pregnancies. There is an increased risk of miscarriage and complications including raised blood pressure.
There is a higher incidence of premature birth. Babies born prematurely may have low birth weight and are at increased risk of still birth and perinatal mortality and if they do live, they may have serious disabilities, such as cerebral palsy and learning problems.
Multiple pregnancies can create the need for extended hospital stay both before and after birth.
A multiple pregnancy and birth can also have a potential strain not only physically but also emotionally, practically and financially on a couple and any existing children.
To minimize the risks of a multiple pregnancy it is important to consider replacing a single embryo (see section 10). The number of embryos that you have transferred will depend very much on your individual circumstances and will be discussed with you in more detail by members of the team. The final decision is not normally made until the day of embryo transfer, when we know exactly how many embryos you have and their quality. However, it is a good idea for you and your partner to start to think now about how you both feel about the risks of multiple pregnancies and how you might cope socially and financially should treatment lead to a multiple birth.
d. Ectopic Pregnancy
Up to 2% of IVF pregnancies implant in the fallopian tubes. This is called an ectopic pregnancy and if left untreated can become life threatening. If you become pregnant following your IVF treatment, we will perform an ultrasound scan to confirm that the pregnancy is in the right place. If you have any pain or bleeding, you must contact the unit.
e. Operative Complications and Infection
IVF does involve invasive surgical procedure and is therefore not without risk. The major risks relate to bleeding at the time of the egg collection and possible pelvic infection afterwards. The incidence of both of these complications is thankfully very low.
Contact Us
If you feel at any time that you are not happy with any aspect of your treatment, have concerns or would like to make a comment or suggestion and would like to discuss things further. Please do not hesitate to contact us as there will always be someone happy to help.
Or in the case of an EMERGENCY please call 0191 482 0000 and ask for a member of the IVF on call team after office hours.
It is very important that you inform the unit about the eventual outcome of the treatment. This is to ensure that we can keep our records up to date but also to allow us to inform the HFEA about the outcome of your treatment.