This information leaflet is to explain what will happen during a Donor Insemination Cycle.
Treatment Cycle
Before the treatment begins you will have selected a sperm donor. The sperm will be stored in our laboratory ready for use. After you have undergone the necessary counselling and signed relevant consent forms you will be able to start your treatment with Day 1 of your period. We are able to offer natural and stimulated cycles, and this will be discussed and agreed by the doctor at your consent appointment.
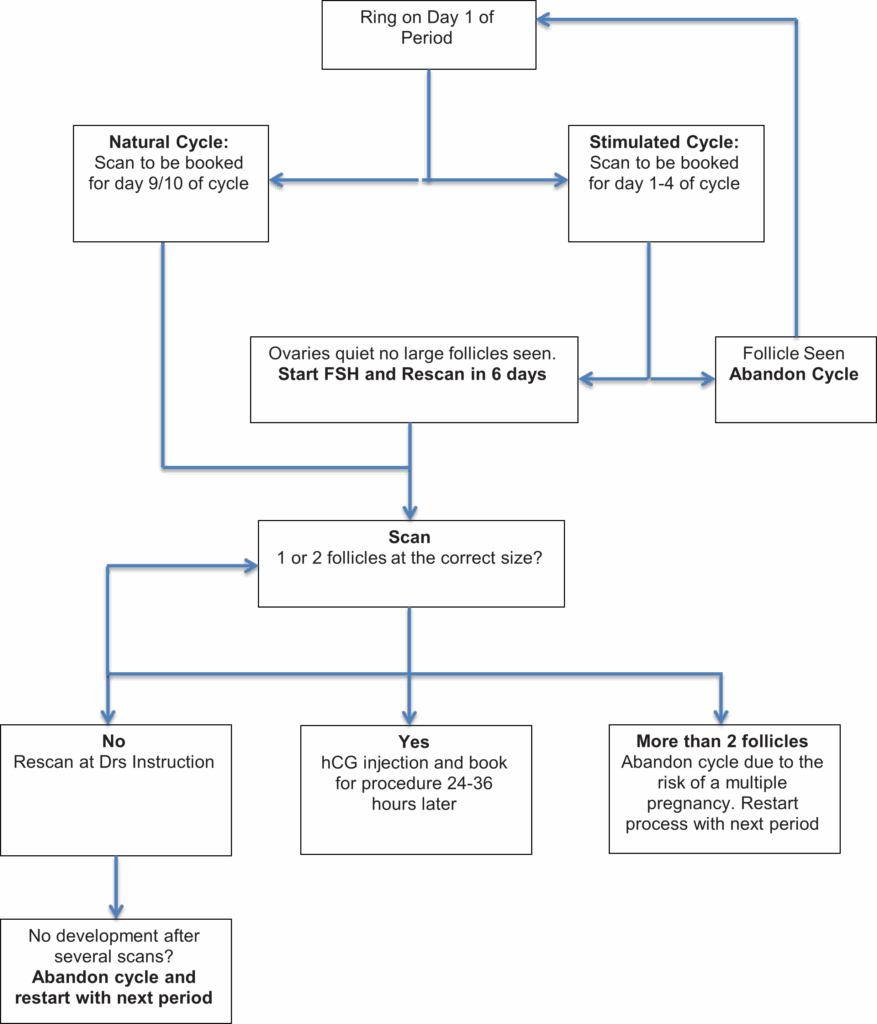
Natural Cycle
Your cycle will be tracked using ultrasound scans until 1 or 2 follicles reach the correct size. Once this has been achieved an injection of human chorionic gonadotrophin (hCG) will be given to start ovulation.
Simulated Cycle
Fertility drugs (FSH) are used to stimulate the growth of one or two follicles and ultrasound scans allow us to monitor the growth of these follicles. Once the largest follicle reaches the correct size, an injection of human chorionic gonadotrophin (hCG) will be given to release the egg(s) from the follicle(s).
In both cycles the insemination will be performed between 24 and 36 hours following hCG injection.
The Procedure
DI is a relatively painless procedure that is performed by the fertility nurses or one of the doctors. Using a speculum, the cervix is cleaned, and a fine catheter is passed through the cervix into the womb – this usually feels similar to a smear test. Next, the prepared sperm sample is placed into the womb through the catheter. You may feel some period-like cramps. After the procedure you will rest for at least 15 minutes before going home.
A urine pregnancy test will be performed at 14 days following the procedure. If your pregnancy test is positive, a blood test will be performed and then a transvaginal scan two weeks later and again at four weeks.
If you have a period or your pregnancy test is negative, you may start the cycle again or you may wish to wait for another period at a time that is suitable for yourself. Whichever you decide you need to contact the unit so that the appropriate appointments can be made.
Problems that can occur
Over stimulation
This occurs in 6-7% of patients taking fertility drugs. In such cases the treatment cycle will have to be abandoned to avoid high order multiple pregnancy.
Multiple Births
The use of fertility drugs increases the risk of a multiple pregnancy by 20-30% as more than one egg follicle may grow. The risk of multiple pregnancies depends on various factors.
The complications of pregnancy increase with multiple pregnancies. There is an increased risk of miscarriage and complications including raised blood pressure.
There is a higher incidence of premature birth. Babies born prematurely may have low birth weight and are at increased risk of still birth and perinatal mortality and if they do live, they may have serious disabilities, such as cerebral palsy and learning problems.
Multiple pregnancies can create the need for extended hospital stay both before and after birth.
Multiple pregnancy and birth can also have a potential strain not only physically but also emotionally, practically and financially on a couple and any existing children.
To avoid this, cycles are strictly monitored by ultrasound scanning and if more than 3 follicles are developing, the cycle is abandoned.
Occasionally, no follicles may grow to be the size required to proceed with ovulation. In this situation, treatment would be abandoned and could restart with the next period. In subsequent cycles it may mean having a stimulated cycle rather than a natural cycle or increasing the dose of FSH in a stimulated cycle.
Chances of Success
At present women under the age of 35 achieve a clinical pregnancy rate of 20.6% per treatment cycle here at the Gateshead Fertility Unit. Nationally the statistic is 17.7% (HFEA 2019).
Websites
You may find the following websites helpful:
www.dcnetwork.co.uk
www.hfea.gov.uk
Step by Step