This leaflet aims to help you understand and gain the maximum benefit from your operation. It gives advice and will help you manage and treat your symptoms. If after reading this leaflet you have any questions, please get in touch.
What is cubital tunnel?
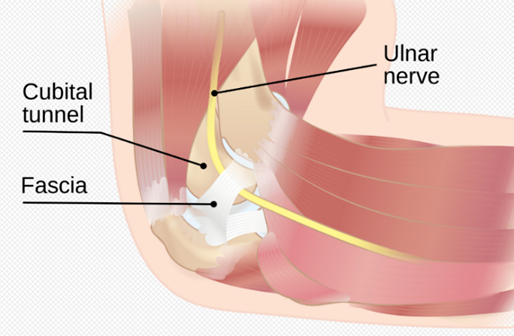
Cubital tunnel syndrome is a condition which affects the ulnar nerve, which is one of the main nerves of your arm and hand. It is responsible for supplying feeling (sensation) to the little finger and half of your ring finger as well as the strength to the small muscles of the hand.
The ulnar nerve travels around the back of the inner side of the elbow and goes through a tight tunnel between the forearm muscles. The nerve can be stretched when the elbow is bent and it can become compressed or irritated within the tunnel. This can cause pins and needles and numbness in your little and ring fingers.
What causes cubital tunnel syndrome?
In most cases there is no obvious reason for cubital tunnel syndrome. Other causes include:
- Direct trauma or a previous elbow injury
- Excessive or repeated bending of the elbow
- Prolonged periods of keeping your elbow in one position ie: when on a phone or sleeping
- Other pre-existing medical conditions such as: diabetes, underactive thyroid, osteoarthritis
Signs and symptoms of cubital tunnel
- Numbness and pins & needles in the little finger and half of the ring finger are common. Often these symptoms will come and go. They occur when the elbow is bent, leaning on the elbow or they may wake you up at night with numbness in the fingers.
- You may feel pain over the inside of the elbow or in the forearm wrist and hand.
- You may notice reduced power and grip strength.
- In severe cases, you may notice muscle wasting at the back of your hand.
Diagnosis of cubital tunnel
Diagnosis can usually be made through clinical examination alone. Further tests may be required called nerve conduction studies. In this test, small electrodes (wires) are placed on your skin to release tiny electric shocks to stimulate the nerves. In the early stages, the test maybe normal although you may still have symptoms of cubital tunnel syndrome. If used, the test can give an indication about the severity of the condition and diagnose other conditions which may be confused with this.
What are the treatment options?
In the early stages and when there are mild to moderate symptoms, the condition can be easily treated.
- Avoid or modify any activity that aggravates your symptoms. Avoid repeated elbow bending like when you are on the phone or resting your elbow on a firm surface.
- Wearing an elbow splint at night can keep the elbow in a slightly bent or neutral position which can reduce the pressure on the nerve. This may involve a specific elbow splint, tapping and using a towel to prevent the elbow from bending.
- In severe cases or when symptoms do not respond to the above measures then surgery may be recommended.
Alternatives to surgery
In mild cases when there is no weakness or permanent numbness the symptoms may improve on their own without surgery. If your symptoms are not severe it is not unreasonable to wait and see if they get better. If symptoms are severe meaning the numbness is there all the time or there is weakness in the hand, then not treating it is likely to lead to worsening symptoms and hand function. The longer the nerve is compressed and the more severe symptoms, the less likely the nerve will make a full recovery after the operation.
Benefits of surgery
The purpose of cubital tunnel release surgery is to improve symptoms and prevent further damage to the nerve. If you have the operation early enough, the numbness in your hand may get better.
What will happen if I don’t have surgery?
If the nerve compression is severe and you have constant numbness or weakness in the hand and you do not have treatment, the nerve may become permanently damaged. This may cause the small muscles in the hand to have wastage and they may become weak, making it difficult to perform tasks such as doing up buttons and tying shoelaces. At this stage, we cannot guarantee the outcome of the surgery and improvement of symptoms. In severe cases, the fingers may also become clawed.
What does the surgery involve?
Cubital tunnel surgery is a day case procedure which means you go home on the same day. It is usually done under a general anaesthetic (you go to sleep) or regional anaesthetic (nerve block but you remain awake). In some cases it is performed under a local anaesthetic. You will discuss with the surgeon or anaesthetist which anaesthetic is best for you. It can take up to 24 hours before the nerve block completely wears off, during this time, you will not be able to move your arm and you may have altered sensation of the arm or hand that persists for some weeks.
Surgery time is up to 45 minutes. On the day of surgery, one of the members of the surgical team will meet you to explain the procedure and will go through the benefits and risks of the operation. You will be asked to sign a consent form.
An incision approximately 4-5 inches is made overlying the inside part of your elbow (near the funny bone). Areas of compression over the nerve are released to create space for the nerve. Your surgeon may perform an ‘ulnar nerve transposition’. This is when the ulnar nerve is moved from behind the bony prominence on the inside of the elbow to lie in front of it; in a position where it is not irritated or pinched. If you need this, the surgical team will discuss this with you. The incision site is closed using internal, absorbable stitches and your elbow will be placed in a dressing with a wool and crepe bandage.
Are there any complications with this operation?
All surgical procedures are associated with a degree of risk. The main complications are:
General complications:
- Pain levels felt after surgery vary for everyone. You will be advised on pain relief after surgery.
- Bleeding (<1%)during or after surgery. This is not usually serious but can cause a haematoma (painful swelling) that takes 1-2 weeks to settle.
- Scarring – unsightly scarring of your skin
- Wound complications including Infection (<1%). You may require antibiotics. Please get in touch on the telephone number below if you suspect you have an infection following surgery.
- Stiffness of the elbow. This usually improves with exercises.
Specific complications:
- Nerve injury or blood vessel injury (<1%) this may cause persistent numbnessin your little and ring finger(s) caused by damage to the nerve during the operation. This can be temporary or permanent.
- Extreme scar sensitivity – thisis common and can be present for to 2-4 months post-surgery.
- Nerve recovery is variable and symptoms may not fully resolve. Wasted hand muscles may never fully recover. The final amount of nerve recovery is around 1 year after the operation.
- Revision surgery due to reoccurrence of symptoms (<3%).
- Persistent symptoms (<5%)your symptoms usually improve within 3 to 4 weeks after the operation but in some cases, often those with more severe nerve damage, it may not improve. There is a small risk that symptoms may be worse due to dissection around the nerve.
- Complex regional pain syndrome (CRPS) (<1%) very rarely you may develop CRPS which can cause swelling and severe, debilitating pain. This is a difficult condition to treat and may last for serval years.
- Anaesthetic complications – the anaesthetist will discuss this with you.
What happens before the operation?
Pre-admission assessment
This is an assessment of your health to make sure you are prepared for your admission, treatment and discharge. Please bring a list of all your current medication including a list of allergies and the type of reactions. Before the date of your admission please, read very closely, the instructions given to you by the pre-admission assessment and your confirmation appointment letter.
Planning ahead
Once you have your date for surgery, you can do several things to aid preparation for your operation and to improve your recovery. It is important to plan and arrange for how you will manage when home. Stocking up your freezer with easy cook items is advised (particularly if you live alone), as you may find daily tasks such as cooking more difficult initially after your operation. If you have family or friends, who can stay with you or visit regularly, this may make your recovery easier both for helping with household tasks and moral support.
Smoking
Smoking is shown to delay wound healing and increase complications after surgery. Patients, who stop smoking benefit from long-term improvements to general health, decrease the risks associated with anaesthetic and may have a better outcome from the operation. If you are interested in stopping smoking, please speak to your pre assessment nurse or GP for advice and services available.
Weight
Even though you may feel fit and healthy at your current weight, patients with a higher body mass index are most likely to experience potential serious complications both during and after surgery. If you are keen to lose weight, please speak to your GP or pre assessment nurse for services available.
Cancellation
If you are unable to attend your appointment, please contact us immediately so that we can offer your appointment to another patient.
Your surgery
Day of surgery
You will be given specific instructions about when to stop eating and drinking, please follow these carefully as otherwise, this may pose an anaesthetic risk and we may have to cancel your surgery. You should bath or shower before coming into hospital. Please remove all rings and jewellery from the arm you are having the operation on.
The anaesthetist, surgeon or a member of the team will visit you prior to the operation and can answer any questions and discuss your anaesthetic with you. You are asked to sign a consent form.
Depending upon the type of anaesthetic used, prior to and during the operation, a blood pressure cuff is placed on your arm, some leads placed on your chest and a clip attached to your finger. This will allow the anaesthetist to check your heart rate, blood pressure and oxygen levels during the operation. With a general anaesthetic, a needle will be put into the back of your hand to administer the drugs to send you to sleep.
Recovery after surgery
Recovery
Many patients notice an improvement of the pins and needles and numbness of the ring and little fingers soon after surgery. However, recovery can be much longer up to 6-12 months depending upon the severity of symptoms.
Wound
After surgery, you will be given advice of rest and elevation of your hand in the sling for 2-3 days after surgery. The wound will be closed with absorbable stitches and you will have a bulky bandage applied after the operation. Leave this in place until you are advised to remove which is usually after 48-72 hours but leave the small dressing on over your wound. Keep the wound clean and dry until you have a GP practice appointment for a wound check which is usually 10-14 days after surgery.
Pain
Although the operation is to relieve symptoms it may be several weeks before you begin to feel the benefit. It is advised to take some simple painkillers such a paracetamol and ibuprofen which should be suitable to relieve this discomfort. If you feel you are unable to manage your pain, please discuss this with your GP or consultant.
Exercises following surgery
After surgery you will need to do some gentle exercises to prevent your fingers, elbow and shoulder from becoming stiff. It is normal for you to feel discomfort or stretching sensations in the elbow when doing these exercises. By 6 weeks following the operation your elbow should be moving normally. If this is not the case, please contact us directly for further advice using the number(s) below.
Repeat approximately 4 x per day or as pain allows
- Wrist – bend your wrist back and forth, repeat x 5
- Fingers – make a fist and then straighten your fingers, repeat x 5
Elbow

Bend and fully straighten your elbow
You can do this assisted initially and then move the elbow on its own.
Repeat each movement x 5


Rest your forearm on a flat surface. Try to turn you palm up towards the ceiling.
Then turn the palm down.
Repeat each movement x 5
Shoulder

Ensure you move your shoulder especially in the first few days after surgery. You can do this assisted if needed.
Repeat x 5

Shrug your shoulders up towards your ears and then back down.
Repeat x 5
Caring for your scar
Your scar maybe sensitive to touch while it is healing. You can start to massage your scar once the wound has fully healed for approximately 8 weeks. This will help to soften the scar and reduce the sensitivity. Use non-perfumed moisturising cream such as E45, aqueous or Vaseline.
Return to activities
You should return to normal everyday activities as your pain allows, often this is around 1-2 weeks after your surgery. Avoid any heavy lifting with the arm for 4-6 weeks.
Driving
You will not be able to drive after surgery. You can return to driving when it is comfortable and safe to do so. You must feel that you are in complete control of the car. Your insurance company should be informed about your operation. Some companies will not insure drivers for several weeks after surgery, so it’s important to check what your policy says.
Return to work
This will depend upon your occupation and, or your place of work. Most people can return to work 2-4 weeks following surgery, but it depends on the type of work you do. For heavy manual work this may be delayed until at least 6 weeks after the operation.
Telephone numbers
| Ward 28 – Contact Level 3, Peter Smith Surgery Centre, Queen Elizabeth Hospital | 0191 445 2028 |
| During the hours of 8am – 8pm contact the Day Surgery Unit, Peter Smith Surgery Centre, Queen Elizabeth Hospital | 0191 445 3009 |
| Main Switchboard | 0191 482 0000 |