This booklet has been produced by the Trauma and Orthopaedic Department. It is designed to provide information about anterior cruciate ligament reconstruction or repair in the knee and what to expect before and after the operation.
This advice is provided to assist with shared decision making when singing informed consent for surgery and help to prepare for surgery, recovery and rehabilitation. It is recommended that you read this booklet before your surgery and write down any questions you may have. You should bring it with you when you come to the hospital.
Anatomy
The knee joint is one of the largest and most complex joints in the body. A joint is formed where two bones meet. The ends of the bones, which form the joint, are covered in articular cartilage. This provides a smooth, slippery and low friction surface that also cushions the joint. Healthy cartilage absorbs stress and allows the bones to glide across each other smoothly.
The knee is made up of the lower end of the thigh bone (femur) which rotates on upper end of the shin bone (tibia). The kneecap (patella) slides in the trochlea grove at the front of the femur as the patellofemoral joint. Large ligaments attached to the femur and the tibia provide stability. The long thigh muscle gives the knee strength.
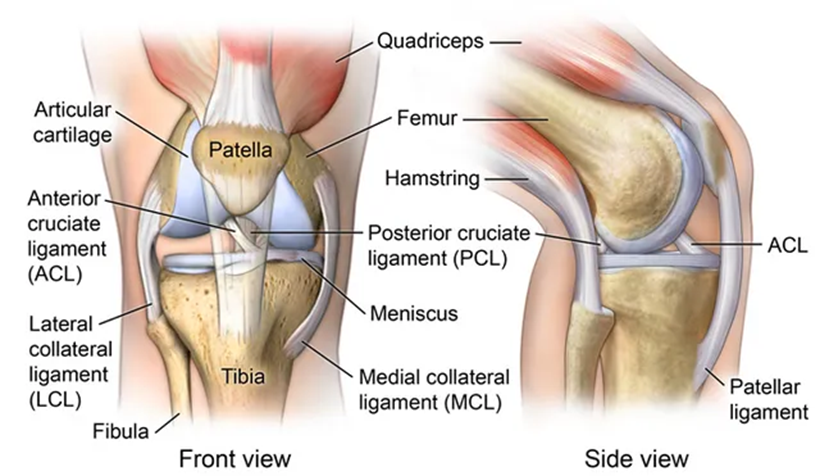
The Anterior Cruciate Ligament (ACL)
The ACL is one of the most important and commonly injured ligaments within the knee. The ACL is a tough band of connective tissue which restricts the tibia (lower leg long bone) moving forward on the femur (thigh bone) and rotating. It runs diagonally through the middle of the knee and gives the knee joint about 85% of its stability.
An ACL rupture (completely torn ligament) is likely to cause instability (giving away sensation), as the restraining mechanism to movement will have been significantly damaged. This can cause symptoms while playing sports but also some basic activities of daily living (washing, dressing, stairs and walking).
Common causes of an ACL injury include:
- Knee twisting when landing from a jump
- Changing direction suddenly e.g. when side stepping
- Stopping suddenly
- During a collision, such as during a football and rugby tackle
Do I need to have an ACL Reconstruction?
Not all patients will have recurrent instability or giving way within the knee following an ACL rupture. It is entirely reasonable to firstly undergo a period of physiotherapy to strengthen your thigh muscles, core stability and improve balance. Following this a proportion of patients will continue with work and undertake activities reasonably symptom free.
ACL reconstruction may be recommended if:
- You’re an athlete and want to continue in your sport, especially if the sport involves jumping, cutting or pivoting
- More than one ligament is injured
- You have a torn meniscus that requires repair
- The injury is causing your knee to buckle during everyday activities
- You’re young (though other factors, such as activity level and knee instability, are more important than age).
How you prepare for surgery?
Before your surgery, it is recommended that you undergo several weeks of physiotherapy. The goal before surgery is to reduce pain and swelling, restore your knee’s full range of motion, and strengthen muscles. People who go into surgery with a stiff, swollen knee may not regain full range of motion after surgery.
ACL reconstruction is a day case procedure, so you’ll be able to go home the same day. Arrange for someone to drive you home. It is recommended to have adult companion at home with you after having an anaesthesia for the procedure.
What does the surgery involve?
The surgery is aimed at replacing the torn ACL with a ligament graft. A number of different tissues can be used to replace your ACL which includes using either:
- part of your hamstring tendons – these run from the back of your knee on the inner side, all the way up to your thigh. Only one or two of the four tendons is used.
- a strip of your patella tendon – this is the tendon running from the bottom of the kneecap (patella) to the top of the shin bone (tibia) at the front of your knee.
- part of your quadriceps tendon – this is the tendon that attaches the patella to the quadriceps muscle, which is the large muscle on the front of your thigh.
- a synthetic graft – this is a tubular structure designed to replace a torn ligament and is commonly made of a type of polyester.
There are various ways of reconstructing the ACL and your surgeon’s team will discuss this with you.
Procedure
The graft is placed in the knee joint and passed through tunnels made into the bones and held in position with fixation devices such as endo button or screw. The procedure is mostly done through keyhole surgery (arthroscopy), though an additional small cut is made to take the graft. Any other procedure needed to address other damage to the knee is usually done at the same time.
What are the risks of surgery?
All surgeries have a potential for complications and whilst this section is not intended to scare you as a patient, it provides information to help you to make an informed decision in the consent process.
It is important that you understand the possible risks linked with any major operation.
Your surgeon or the member of the orthopaedic team will discuss the operation during the consent process and typically would list the following potential complications on the consent form, “infection, damage to nerves and vessels, thromboembolism, pain, stiffness, swelling, graft failure, further surgery, risks to limb or life”. You will be asked to sign the consent form stating that you understand and are accepting the risks when undergoing surgery. You can withdraw from a surgery at any point of time if you have changed your mind.
Possible complications are listed below:
- Infection – can occur with any operation. Special precautions are taken to reduce this risk. The infection risk is low less than 1 in 100 (1%) and can usually be treated with antibiotics. In some cases it may be necessary to perform further surgery.
- Damage to nerves and vessels – The surgery is carried out next to a number of nerves and blood vessels. Injury to these nerves or vessels occurs in less than one in 100 patients. Its normal to experience loss of sensation to touch surrounding your scars which usually decrease over the time.
- Blood clots in your leg (deep vein thrombosis DVT) – This can cause pain, swelling or redness in your calf. This is rare particularly if you mobilise early as instructed by the physiotherapists. A blood clot if left untreated can become serious please see medical advice if concern.
- Stiffness – Post-operative stiffness can occur as the knee responds to the trauma of the surgery.
Sometimes, scar tissue builds up inside the knee, restricting your movement. Some patients may struggle to regain the ability to fully straighten the knee. Good physiotherapy rehabilitation will assist in decreasing the risks and improve your recovery. - Pain – Pain can happen with any operation. A local anaesthetic is given during surgery to help control your post-operative pain and you will have pain relief to go home with. Should there be arthritis found within your knee you may continue to get pain.
- Graft failure/ re-tear – There are number of reasons as to why the surgical graft may fail or you may suffer a re-tear of the ACL. Failure of the graft can occur if excessive force occurs to
the knee around 1 in 20 (5%). This can cause you to have recurrence of your symptoms. There is a small risk of gradual stretching of the graft which can cause you to have recurrence of your instability symptoms. Physiotherapy exercises are designed to help reduce this risk. - Compartment syndrome – can occur as a result of increased pressure around the muscles of the lower leg as a consequence of bleeding or swelling. This requires extended hospital stay for monitoring and may mean further surgery on your lower leg to release the pressure. The risk
to you is less than 0.1%. - Instability
- Arthritis
What happens after surgery?
When you wake up, you will have a bandage and you may have a special brace around your knee. If you have had other procedures in combination with your ACL reconstruction, for example, a meniscal repair, you may need to keep this on for up to 6 weeks. You will have a wound that will require some nursing care at 2 weeks after surgery. You must keep this clean and dry until you are asked to see your practice nurse at your GP surgery. Your brace (if you were advised to use one) is designed to restrict movement at certain intervals and you will be asked to wear it at all times for the first 4 or 6 weeks. It should be adjusted at particular time scales in your recovery – your doctor, physiotherapist or advanced practitioner will explain this to you as applicable.
You may be asked not to weight bear on your operated leg or to put partial weight through it when you walk. Both of these requirements mean you will need to use 2 crutches at all times. The physiotherapy team on the ward will talk to you about this. Sometimes you are allowed to weight bear again after 2 weeks. Sometimes we do not restrict you at all. This will be explained to you directly as each case is individual.
You should be prepared to take your recommended pain relief regularly and as advised by your medical team. The immediate few weeks after surgery can be difficult in terms of controlling your pain and swelling. You must also be prepared to work hard at the physiotherapy exercises given to you at the appropriate stages in your recovery.
Swelling and bruising
Due to the nature of the surgery, there will be some swelling in the knee, which will go down over the time. Sometimes, initial bruising can happen, but should settle quickly. Ice packs and high elevation with your leg above the height of your pelvis can help. Do that regularly in the first 6 weeks of your recovery.
Ice should not be directly placed onto the skin. An ice pack or a bag of frozen peas should be wrapped in a pillowcase or a cloth to prevent you burning the skin. Ice packs should only be applied for short intervals of 10-15min at a time, to prevent causing further tissue damage and more swelling. Do not elevate your leg on a low foot stool.
Following surgery, your knee gradually heals over the course of 6-9 months. You will be seen in outpatient’s clinic a few weeks after your operation and then followed up until your surgeon is satisfied with your level of recovery for you to be discharged.
Driving
You must not drive for 6 weeks following your surgery. Doing so may render your insurance policy invalid. After this you may drive when you are comfortable and safe to do so. Ideally, you will have stopped using crutches and be able to sit comfortably. You should have enough power and bend in your knee to perform an emergency stop. You may get back to driving quicker if you have an automatic car. The law states you should be always in complete control of your car. It is your responsibility to ensure this.
Returning to work
You are likely to be away from work for anywhere up to 3 months after surgery. This largely depends on what sort of job it is you do. Desk based workers can often return before, however you should remember that prolonged standing or sitting can make your knee swell and increase your pain.
Patients with a more manual profession such as builders or other manual trades may not be fully operational for 4-6 months. Your consultant’s team will advise you.
Sports & Exercise
Your return to leisure activities will be guided by your surgeon and physiotherapist and will depend on how you are progressing, type of graft used and whether you are reaching certain goals.
Your physiotherapist will advise you when you are physically capable to deal with different activities and will ensure you progress to a level where it is safe for you to return to certain activities. It is vitally important that the rehabilitation programme is followed and that a return to sport does not occur until your physiotherapist agrees. Usually return to sport is advised between 9 and 12 months.
Further reading/links
NHS Knee ligament surgery https://www.nhs.uk/conditions/knee-ligament-surgery/